We use a two stage approach to assess the needs of the communities where we operate Child Health programs.
1. Qualitative Problem Trees
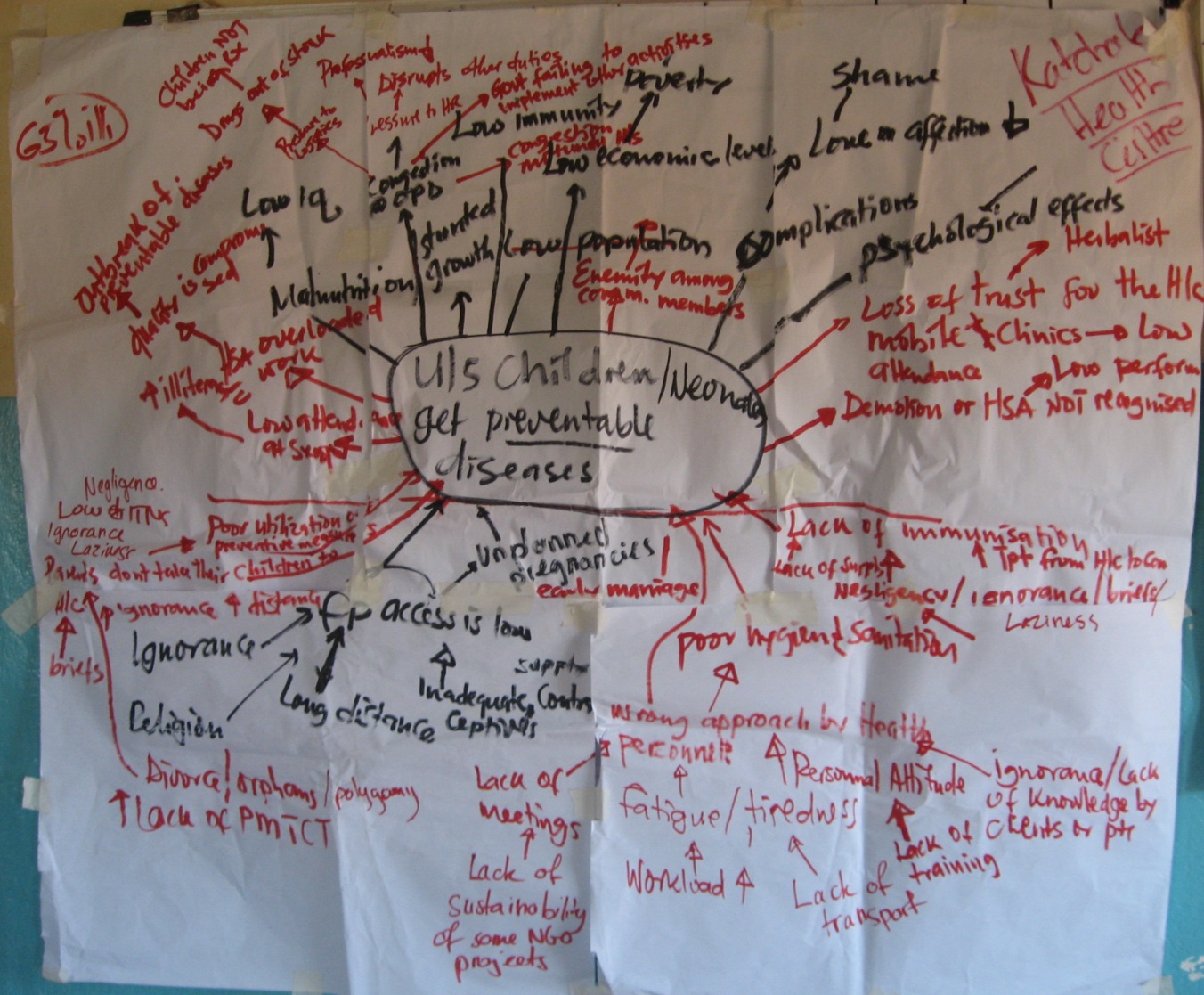
Problem tree created by health workers at Katchale Health Centre
We begin by running a series of meetings with community representatives, local chiefs, Health Centre staff and Health District Office staff. During each meeting groups are asked to create a problem tree showing what they thought are the root causes of child morbidity and mortality.
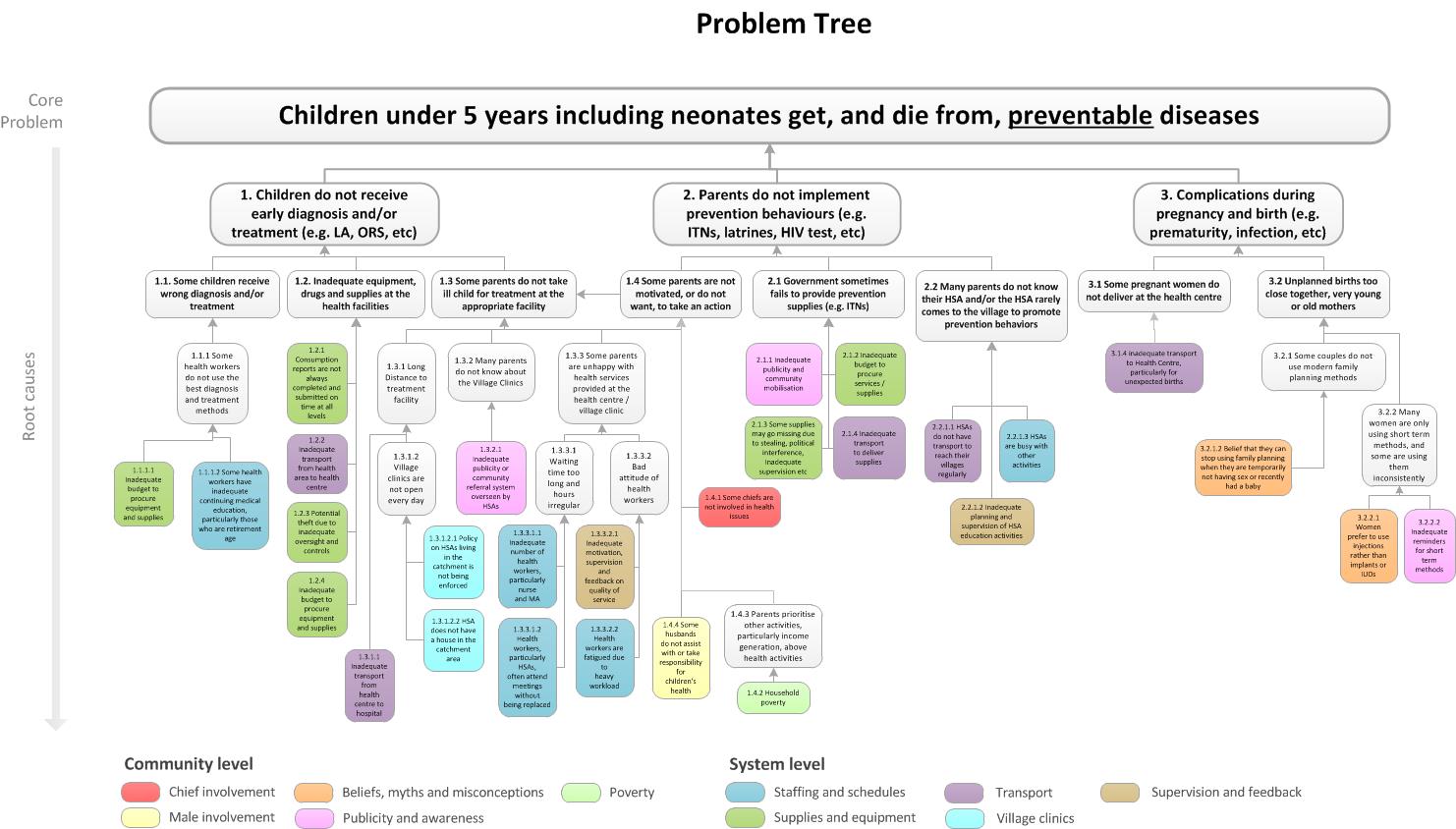
The separate problem trees are then combined to produce a final problem tree, such as the one shown below. Review meetings are then held with the Traditional Authority, Area Development Committee, District Health Office and Health Area to validate the final problem tree.
Common problems identified at the community level:
- Chiefs not fully involved in health issues
- Beliefs, myths and misconceptions about health
- Inadequate male involvement
- Inadequate publicity and awareness
- Poverty
Common problems identified at the Health System level:
- Inadequate staffing and inefficient scheduling
- Inadequate supplies and equipment
- Inadequate transport
- Health workers not living in the village clinic catchment areas
- Inadequate supervision and feedback for health staff
For further details see the Program Documents for each Child Health Program that can be found in the Document section.
2. Quantitative Baseline Survey
Following the creation of a problem tree, the next stage in the process is to conduct a baseline survey (see Documents). This is conducted to validate the problems identified in the problem tree.
The results of the baseline survey are used to update the final problem tree. Problems that are not validated are removed, while some additional problems discovered during the baseline may be added.
All baseline survey results are analysed and presented within a Baseline Survey Report – these reports can be found on the Documents section of this site. An example of a final problem tree from Katchale (Central Region) is shown below: